

Health
Understanding a Treatment Option for Advanced Kidney Cancer

(Family Features) When kidney cancer spreads or becomes advanced, it can be challenging to treat. Common signs and symptoms can include blood in urine, lower back pain on one side, a mass on the side or lower back, loss of appetite or unexplained weight loss.
While a diagnosis of advanced kidney cancer can be overwhelming, there are steps patients can take to feel more empowered as they face the disease, starting with learning about the treatments that may be available for them.
Exploring Your Options
When facing advanced kidney cancer, it’s important for patients and caregivers to have open communication with their healthcare team to understand the diagnosis and establish a treatment plan.
Asking questions to understand where the cancer has spread, what the expected prognosis is and the potential benefits of treatment – including the possibility to live longer – can be critical to aligning on a path forward.
Fortunately, there are several types of medicines available for advanced kidney cancer today, depending on the specifics of each patient’s disease. Chemotherapy, targeted therapy or immunotherapy are a few types of treatment that may be considered, sometimes in combination. Immunotherapy works differently than chemotherapy or targeted therapy, as it helps a person’s own immune system to fight cancer and can enable the immune system to find and attack cancer cells. For some patients, dual immunotherapy – or a combination of two immunotherapy treatments – may be recommended.
For example, Opdivo (nivolumab) + Yervoy (ipilimumab) is approved by the U.S. Food and Drug Administration (FDA) as a combination of two immunotherapies for certain newly diagnosed adults whose kidney cancer (also referred to as renal cell carcinoma) has spread. It is not known if Opdivo is safe and effective in children younger than 18 years of age. Opdivo (10 mg/mL) and Yervoy (5 mg/mL) are injections for intravenous use.
This combination of two immunotherapies has the potential to work with the immune system in different but complementary ways to help fight cancer. While Yervoy may stimulate the kind of cells that help fight cancer, Opdivo may help these cells find and fight the cancer cells again.
While doing so, this immunotherapy combination can also affect healthy cells. These problems can sometimes become serious or life threatening and can lead to death. These problems may happen anytime during treatment or even after treatment has ended. You may have more than one of these problems at the same time. Some of these problems may happen more often when Opdivo is used in combination with Yervoy.
Opdivo and Yervoy can cause problems that can sometimes become serious or life-threatening and can lead to death. Serious side effects may include lung problems; intestinal problems; liver problems; hormone gland problems; kidney problems; skin problems; eye problems; problems in other organs and tissues; severe infusion reactions; and complications of stem cell transplant, including graft-versus-host disease (GVHD), that uses donor stem cells (allogeneic). Call or see your healthcare provider right away for any new or worsening signs or symptoms. Please see additional Important Safety Information below.
Understanding Overall Survival
One of the most important considerations for choosing a treatment is the potential for survival, or the chance to live longer. Overall survival is sometimes reported as a survival rate, which is the percentage of people in a clinical trial who are still alive for a certain time period after being diagnosed with or starting treatment for a disease, such as cancer.
“After my cancer diagnosis, my wife and I prayed about our future and pursuing every avenue with that goal in mind,” said Terry Broussard, who has been living with advanced kidney cancer. “I wanted a treatment that may give me a chance to live longer in order to see my youngest child graduate high school.”
Broussard’s doctor recommended treatment with Opdivo + Yervoy, which has overall survival data at five years. The FDA approval of this dual immunotherapy in advanced renal cell carcinoma (RCC) was based on results from the CheckMate -214 clinical trial, which included 847 previously untreated patients with kidney cancer that had spread and with one or more risk factors.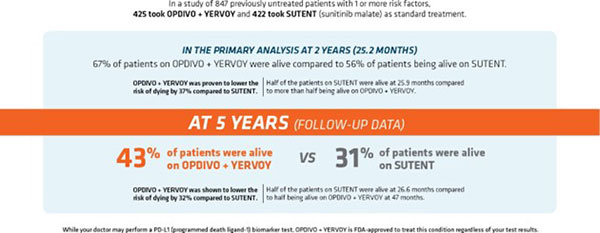
In the primary analysis at two years (25.2 months), the length of time patients lived without tumors worsening was 11.6 months for this immunotherapy combination and 8.4 months for sunitinib. There was no meaningful difference between the two treatments.
Researchers also assessed the overall response rate, which is a measure of the percentage of patients whose cancer shrunk (partial response) or disappeared completely (complete response) after treatment.
At the two-year time point, 41.6% of patients treated with Opdivo + Yervoy (95% CI:36.9-46.5) responded to treatment (n=177/425) versus 26.5% (n=112/422) of those treated with sunitinib (95% CI:22.4-31.0). Partial tumor shrinkage occurred in 32.2% of the patients treated with this immunotherapy combination compared to 25.4% of those treated with sunitinib. Tumors disappeared completely in 9.4% of patients treated with this immunotherapy combination versus in 1.2% of patients treated with sunitinib. The disappearance of any measurable tumors in response to treatment does not necessarily mean the cancer has been cured. Opdivo + Yervoy will not work for everyone. Individual results may vary.
“Advanced kidney cancer is a complex disease with many treatment options, which can feel overwhelming for people facing a devastating cancer diagnosis,” said Ulka Vaishampayan, M.D., professor, Internal Medicine, Division of Hematology/Oncology, University of Michigan. “The goal of treatment is to help patients live longer, and research like these five-year data gives us insight into what treatment with Opdivo + Yervoy may look like for patients from the trial over time.”
The most common side effects of Opdivo, when used in combination with Yervoy, include: feeling tired; diarrhea; rash; itching; nausea; pain in muscles, bones, and joints; fever; cough; decreased appetite; vomiting; stomach-area (abdominal) pain; shortness of breath; upper respiratory tract infection; headache; low thyroid hormone levels (hypothyroidism); constipation; decreased weight; and dizziness.
Establishing and Leaning on a Support System
From diagnosis to treatment and beyond, many patients find the support from family, friends and loved ones invaluable. Identifying a friend, spouse or caregiver who can join doctor appointments, ask questions and take notes can be a helpful way to track all the details that can often be overwhelming when facing cancer. “I’ve been incredibly lucky to have the support of my wife, children, nurses and doctors every step of the way,” said Broussard. “Even in the most challenging moments, knowing they were by my side gave me the hope and inspiration I needed to continue moving forward.”
To learn more, visit Opdivo.com.
Source: Bristol Myers Squibb
Photo caption: Terry Broussard and his wife, Tracy. Broussard is an actual patient who has been compensated by Bristol Myers Squibb for his time.
INDICATION AND IMPORTANT SAFETY INFORMATION
OPDIVO® (nivolumab) is a prescription medicine used in combination with YERVOY® (ipilimumab) to treat adults with kidney cancer in certain people when your cancer has spread (advanced renal cell carcinoma) and you have not already had treatment for your advanced RCC.
It is not known if OPDIVO is safe and effective in children younger than 18 years of age.
Information provided in this article is not a substitute for talking with your healthcare professional. Your healthcare professional is the best source of information about your disease.
Important Safety Information for OPDIVO® (nivolumab) + YERVOY® (ipilimumab)
What is the most important information I should know about OPDIVO + YERVOY?
OPDIVO and YERVOY are medicines that may treat certain cancers by working with your immune system. OPDIVO and YERVOY can cause your immune system to attack normal organs and tissues in any area of your body and can affect the way they work. These problems can sometimes become severe or life-threatening and can lead to death. These problems may happen anytime during treatment or even after your treatment has ended. You may have more than one of these problems at the same time. Some of these problems may happen more often when OPDIVO is used in combination with another therapy.
What are the serious side effects of OPDIVO + YERVOY?
Call or see your healthcare provider right away if you develop any new or worse signs or symptoms, including:
- Lung problems: new or worsening cough; shortness of breath; chest pain
- Intestinal problems: diarrhea (loose stools) or more frequent bowel movements than usual; stools that are black, tarry, sticky, or have blood or mucus; severe stomach-area (abdominal) pain or tenderness
- Liver problems: yellowing of your skin or the whites of your eyes; severe nausea or vomiting; pain on the right side of your stomach area (abdomen); dark urine (tea colored); bleeding or bruising more easily than normal
- Hormone gland problems: headaches that will not go away or unusual headaches; eye sensitivity to light; eye problems; rapid heart beat; increased sweating; extreme tiredness; weight gain or weight loss; feeling more hungry or thirsty than usual; urinating more often than usual; hair loss; feeling cold; constipation; your voice gets deeper; dizziness or fainting; changes in mood or behavior, such as decreased sex drive, irritability, or forgetfulness
- Kidney problems: decrease in your amount of urine; blood in your urine; swelling in your ankles; loss of appetite
- Skin problems: rash; itching; skin blistering or peeling; painful sores or ulcers in the mouth or nose, throat, or genital area
- Eye problems: blurry vision, double vision, or other vision problems; eye pain or redness.
Problems can also happen in other organs and tissues. These are not all of the signs and symptoms of immune system problems that can happen with OPDIVO and YERVOY. Call or see your healthcare provider right away for any new or worsening signs or symptoms, which may include:
- Chest pain; irregular heart beat; shortness of breath; swelling of ankles
- Confusion; sleepiness; memory problems; changes in mood or behavior; stiff neck; balance problems; tingling or numbness of the arms or legs
- Double vision; blurry vision; sensitivity to light; eye pain; changes in eye sight
- Persistent or severe muscle pain or weakness; muscle cramps
- Low red blood cells; bruising
Getting medical help right away may help keep these problems from becoming more serious. Your healthcare team will check you for these problems during treatment and may treat you with corticosteroid or hormone replacement medicines. Your healthcare team may also need to delay or completely stop your treatment if you have severe side effects.
Possible side effects of OPDIVO + YERVOY
OPDIVO and OPDIVO + YERVOY can cause serious side effects, including:
- See “What is the most important information I should know about OPDIVO + YERVOY?”
- Severe infusion reactions. Tell your healthcare team right away if you get these symptoms during an infusion of OPDIVO or YERVOY: chills or shaking; itching or rash; flushing; shortness of breath or wheezing; dizziness; feel like passing out; fever; back or neck pain
- Complications, including graft-versus-host disease (GVHD), of bone marrow (stem cell) transplant that uses donor stem cells (allogeneic). These complications can be severe and can lead to death. These complications may happen if you underwent transplantation either before or after being treated with OPDIVO or YERVOY. Your healthcare provider will monitor you for these complications.
The most common side effects of OPDIVO, when used in combination with YERVOY, include: feeling tired; diarrhea; rash; itching; nausea; pain in muscles, bones, and joints; fever; cough; decreased appetite; vomiting; stomach-area (abdominal) pain; shortness of breath; upper respiratory tract infection; headache; low thyroid hormone levels (hypothyroidism); constipation; decreased weight; and dizziness.
These are not all the possible side effects. For more information, ask your healthcare provider or pharmacist. You are encouraged to report side effects of prescription drugs to the FDA. Call 1-800-FDA- 1088.
Before receiving OPDIVO or YERVOY, tell your healthcare provider about all of your medical conditions, including if you:
- have immune system problems such as Crohn’s disease, ulcerative colitis, or lupus
- have received an organ transplant
- have received or plan to receive a stem cell transplant that uses donor stem cells (allogeneic)
- have received radiation treatment to your chest area in the past and have received other medicines that are like OPDIVO
- have a condition that affects your nervous system, such as myasthenia gravis or Guillain-Barré syndrome
- are pregnant or plan to become pregnant. OPDIVO and YERVOY can harm your unborn baby
- are breastfeeding or plan to breastfeed. It is not known if OPDIVO or YERVOY passes into your breast milk. Do not breastfeed during treatment with OPDIVO or YERVOY and for 5 months after the last dose of OPDIVO or YERVOY.
Females who are able to become pregnant:
Your healthcare provider should do a pregnancy test before you start receiving OPDIVO or YERVOY.
- You should use an effective method of birth control during your treatment and for at least 5 months after the last dose of OPDIVO or YERVOY. Talk to your healthcare provider about birth control methods that you can use during this time.
- Tell your healthcare provider right away if you become pregnant or think you may be pregnant during treatment with OPDIVO or YERVOY. You or your healthcare provider should contact Bristol-Myers Squibb at 1-844-593-7869 as soon as you become aware of a pregnancy.
Tell your healthcare provider about all the medicines you take, including prescription and over-the- counter medicines, vitamins, and herbal supplements.
Please see U.S. Full Prescribing Information and Medication Guide for OPDIVO and YERVOY.
© 2023 Bristol-Myers Squibb Company. All Rights Reserved.
OPDIVO® and YERVOY® are registered trademarks of Bristol-Myers Squibb Company.
7356-US-2200719 2/23
SOURCE:
Bristol Myers Squibb
https://stmdailynews.com/category/lifestyle/health-and-wellness/









Health
Truth Initiative and NAACP Expand Partnership to Advance Health Equity and Increase Access to Proven Quit Resources

Health Equity
When we talk about health equity, we’re really talking about who gets the chance to live a longer, healthier life — and who has been systematically denied that chance. Tobacco and nicotine addiction remain a clear example of that imbalance, especially in Black communities and other historically marginalized groups.
That’s why Truth Initiative and the NAACP are expanding their partnership to increase access to proven quit support and to reframe nicotine cessation as something bigger than an individual choice. Their new phase of collaboration launches the Breath of Freedom Movement, powered by Truth Initiative and the NAACP — a community-centered effort that combines civil rights leadership with public health expertise.
A movement rooted in community and accountability
The Breath of Freedom Movement builds on the work of the Breath of Freedom coalition, an alliance led by Truth Initiative across Black-led organizations. The coalition’s mission has been to reclaim the narrative around tobacco use, confront the ways the industry has shaped that narrative, and connect people to support that respects culture, history, and lived experience.
This expansion arrives at a critical moment. According to the press release, approximately 45,000 Black Americans die each year from smoking-related illness. The burden is not accidental — it has been driven in large part by decades of targeted marketing of menthol cigarettes and other flavored tobacco products.
The release highlights another stark disparity: more than 80% of Black smokers use menthol cigarettes, compared with 43% of adult smokers overall. Menthol products are often described as easier to start and harder to quit, which makes access to culturally relevant cessation resources not just helpful, but essential.
Launching at the NAACP National Convention in Chicago
The Breath of Freedom Movement will officially launch at the NAACP National Convention, taking place July 18–22, 2026, in Chicago. The convention theme, “We, The People,” commemorates the nation’s 250th anniversary and marks 100 years since Chicago first hosted the NAACP conference in 1926.
As part of the convention programming, Truth Initiative will debut the Rise Together EXperience: Culture, Community, and Nicotine-Free Lives — an immersive mobile exhibit designed to explore how tobacco use and industry marketing tactics have impacted Black, Hispanic, and LGBTQ+ communities. The exhibit is also meant to connect people to quit support in a way that feels accessible and grounded in real community conversations.
What the expanded partnership will do
Truth Initiative and the NAACP say this partnership is designed to move beyond awareness and into action — action that’s rooted in community spaces where trust already exists. The expanded collaboration will focus on:
- Hosting culturally relevant presentations, community forums, workshops, and healing-centered discussions about the health consequences of smoking, vaping, and nicotine addiction, with a focus on disproportionate impacts.
- Advancing the Breath of Freedom mission by reframing nicotine cessation as an act of liberation and resistance to the tobacco industry’s exploitation of Black communities.
- Co-developing and distributing culturally relevant public health content, including toolkits, digital resources, and community-informed cessation materials.
- Promoting awareness of and access to proven quit resources — including Truth Initiative’s EX Program — in partnership with Black-led organizations, faith-based groups, LGBTQ+ advocates, and other culturally aligned stakeholders.
- Strengthening local, regional, and national outreach strategies that elevate community voices and mobilize grassroots support for nicotine prevention and cessation.
In the release, Dr. Chris T. Pernell, Director of the NAACP Center of Health Equity, underscored that health equity requires more than information — it requires accountability and community-rooted action that connects people with tools for healing and freedom from addiction.
Quitting as liberation — not just willpower
One of the most important shifts in this work is the language: quitting isn’t framed as a moral test or a matter of “just trying harder.” Instead, it’s positioned as a supported process — and as a way for communities to push back against systems that have profited from addiction.
As Dr. Dartis noted in the announcement, the tobacco industry has targeted Black communities for generations with products and marketing designed to drive nicotine addiction. The expanded partnership aims to meet people where they are — in trusted spaces, through meaningful conversations, and with resources that recognize culture and lived experience.
Bridging public health data and lived experience
The press release also notes that Dr. Dartis will be featured in an upcoming NAACP docuseries focused on bridging the gap between public health data and the lived experiences of Black men in America. The project will explore the systems, relationships, and environments that shape health outcomes, while highlighting resilience and calling for accountability from the systems meant to serve communities.
How to get free quit support
If you or someone you care about is ready to quit smoking, vaping, or other nicotine products, free support is available through Truth Initiative’s EX Program.
- Text JoinFreedom to 88709
- Visit exprogram.com
Local resources (Arizona)
If you’re in Arizona and want additional, local support, consider these options:
- Arizona Smokers’ Helpline (ASHLine): Call 1-800-55-66-222 or visit https://www.azdhs.gov/ashline/ for free quit coaching and support for Arizona residents.
- Arizona 2-1-1: Dial 2-1-1 (or visit 211arizona.org) to get connected to local health services, community programs, and support resources.
- Primary care clinics and community health centers: If you have a regular doctor or use a community clinic, ask about quit plans and nicotine replacement options. Many clinics can help you build a step-by-step approach and connect you to additional programs.
The takeaway
The Breath of Freedom Movement is a reminder that nicotine addiction doesn’t exist in a vacuum. It’s connected to policy, marketing, access to care, and the long history of unequal health outcomes in the United States. By combining community leadership with proven quit resources, Truth Initiative and the NAACP are working to ensure that communities most impacted by tobacco-related harm have the support they need to heal, quit, and thrive.
Credit: Truth Initiative. News provided by Truth Initiative via PRNewswire, July 17, 2026.
- Related Links
- https://www.exprogram.com (or exprogram.com)
- https://www.azdhs.gov/ashline/
- https://211arizona.org
💪 Your health journey starts here! Explore the latest health news, fitness tips, wellness trends, and healthy living advice. Share your thoughts in the comments and subscribe to the STM Daily News newsletter to stay informed and inspired every day.
Health
Black Girl Sunscreen Founder Shontay Lundy Inducted into Sigma Gamma Rho’s 2026 TrailblazerΣ Honorary Membership Class

Shontay Lundy, Founder and CEO of Black Girl Sunscreen, has been inducted into Sigma Gamma Rho Sorority’s 2026 TrailblazerΣ Honorary Membership Class—an honor recognizing women whose leadership and accomplishments create measurable impact across culture and community.
Announced July 29, 2026, the recognition places Lundy among 21 accomplished women celebrated for reshaping their industries through service, sisterhood, and scholarship. For Lundy, it’s a milestone that reflects not only entrepreneurial success, but also the broader advocacy work that has helped expand how the beauty and skincare world talks about inclusive sun care and representation.

What the TrailblazerΣ Honorary Membership Recognizes
Sigma Gamma Rho Sorority, founded in 1922, is a national collegiate sorority with more than 100,000 members across 500 chapters worldwide. Built on principles of leadership and service, the organization is known for its long-standing commitment to community outreach—captured in its slogan, “Greater Service, Greater Progress.”
Honorary membership is among Sigma Gamma Rho’s most prestigious distinctions. It is awarded to women whose work excels in their field while also positively influencing society at large. The TrailblazerΣ class, in particular, highlights leaders who redefine what’s possible and open doors for others.
A Recognition Linked to a Larger Mission
Lundy founded Black Girl Sunscreen in 2016 to address a persistent gap in the market: sun protection products that work well for people of color, without leaving an unwanted white cast. Since then, the brand has become a recognizable name in inclusive skincare—helping educate consumers on sun safety and shifting public perception around who sunscreen is “for.”
Her induction into Sigma Gamma Rho’s 2026 class connects that work to a larger legacy of women breaking barriers across industries. It also underscores the brand’s impact beyond product innovation—positioning Black Girl Sunscreen as part of a wider movement toward representation, health education, and community-driven leadership.
In a statement, Lundy emphasized that the honor reflects shared values and a commitment to creating opportunities for others:
“To be welcomed into Sigma Gamma Rho is incredibly meaningful because it represents more than recognition—it reflects a shared commitment to service, leadership, and creating opportunities for others. Throughout my journey, I’ve always believed success should open doors, not just for yourself, but for the women coming behind you. I’m honored to join a sisterhood whose legacy is rooted in that same purpose, and I look forward to continuing that work together.”

A Class of Leaders Across Industries
Lundy joins a group of honorees spanning business, sports, media, and public service—reflecting Sigma Gamma Rho’s tradition of recognizing women whose achievements extend beyond personal success to broader community impact.
As the beauty industry continues to evolve toward more inclusive products and messaging, Lundy’s recognition signals how far the conversation has come—and how much it still depends on leaders willing to challenge assumptions, educate consumers, and build brands with purpose.
About Black Girl Sunscreen
Black Girl Sunscreen is a beauty and skincare company founded by Shontay Lundy in 2016 to address the lack of sun protection products formulated for people of color. The brand’s mission centers on educating consumers about safe skin practices and sun protection, while providing premium sun care products formulated for melanated skin and designed to be exceptional for everyone.
For more information, visit blackgirlsunscreen.com.
💪 Your health journey starts here! Explore the latest health news, fitness tips, wellness trends, and healthy living advice. Share your thoughts in the comments and subscribe to the STM Daily News newsletter to stay informed and inspired every day.

Three new studies shared this week at the Society of NeuroInterventional Surgery (SNIS) 23rd Annual Meeting deliver a clear message: stroke care in the U.S. is improving, but those gains are not reaching everyone equally. Researchers found persistent disparities tied to race, geography, and socioeconomic status—factors that can shape whether a patient receives advanced treatment, how quickly they reach specialized care, and ultimately, whether they survive.
Stroke remains one of the nation’s leading causes of death and long-term disability. In recent years, breakthroughs in emergency response systems and minimally invasive procedures have expanded what’s possible in the critical first hours after a stroke. But the latest findings suggest that access to those life-saving advances still depends too heavily on who you are and where you live.
Study 1: Treatment gaps widen as strokes get more severe
The first study, “Racial Disparities in Endovascular Thrombectomy Widen with Stroke Severity: A National Inpatient Sample Analysis,” examined more than 325,000 acute ischemic stroke patients treated at U.S. teaching hospitals between 2018 and 2022.
The focus was endovascular thrombectomy (EVT), a minimally invasive procedure in which specialists remove a clot from a blocked artery in the brain. EVT can be a game-changer for eligible patients—but researchers found Black patients were less likely than white patients to receive it across all levels of stroke severity.
What stood out most: the disparity grew as stroke severity increased. At a National Institutes of Health Stroke Scale (NIHSS) score of 20, the predicted probability of receiving EVT was:
- 33% for white men
- 32% for white women
- 28% for Black men
- 26% for Black women
Co-first author Muhammed Amir Essibayi, MD, MSc, FRCP, noted that timely access becomes even more critical as severity rises—yet the treatment gap becomes more pronounced. The study also highlighted an intersectional pattern, with Black women consistently least likely to receive EVT.
Study 2: Hemorrhagic stroke deaths are falling—but disparities persist
The second study, “Reducing Inequalities in Stroke Events-Hemorrhagic Disparities (RISE-HD): A 10-year Statewide Analysis of Social Determinants of Mortality in Hemorrhagic Stroke,” analyzed more than 120,000 patients hospitalized with hemorrhagic stroke in Florida between 2013 and 2024.
There was good news: mortality rates declined significantly over the decade, suggesting real progress in stroke systems and hospital care.
But after adjusting for age, sex, and comorbidities, disparities remained. Black patients had higher odds of in-hospital mortality than white patients. Higher mortality was also associated with:
- Living in rural areas
- Having Medicaid or other non-commercial insurance
Researchers also found regional differences across Florida, pointing to uneven access to specialized stroke care.
Primary author Natália Vasconcellos, MD, MSc, emphasized that improving outcomes for everyone will require addressing barriers to specialized stroke systems—especially in underserved communities.
Study 3: The “Stroke Belt” has two different access problems
The third study, “Dual Pathways to Hemorrhagic Stroke Mortality Across the U.S. Stroke Belt: Rural Neurointerventional Isolation and Urban Structural Vulnerability,” looked at hemorrhagic stroke mortality across 433 counties in the “Stroke Belt,” a region long associated with higher stroke rates and worse outcomes.
Researchers compared factors linked to mortality in rural versus urban counties, including:
- Distance to the nearest Comprehensive Stroke Center
- Community-level socioeconomic disadvantage
- Racial and economic segregation
- HIV burden
They found the drivers of mortality differed sharply by setting:
- In rural counties, longer travel times to Comprehensive Stroke Centers were more strongly associated with higher mortality.
- In urban counties, racialized economic segregation and HIV burden were more strongly associated with poorer outcomes—even when specialized care was geographically closer.
Dylan Yates, a medical student at Tulane University School of Medicine, summarized the takeaway: the neurointerventional access gap in the Stroke Belt is “not one problem, it is two.” Solutions need to match the reality on the ground—strengthening transfer networks and specialty connections in rural areas, while addressing structural disadvantage and underinvestment in urban communities.
What to watch for: where the system can improve
Across all three studies, the common thread is that medical innovation alone doesn’t guarantee equitable outcomes. Researchers pointed toward targeted interventions that could help close the gap, including:
- More consistent, equitable treatment pathways for advanced stroke procedures like EVT
- Stronger stroke transfer networks to reduce delays—especially in rural regions
- Expanded access to specialty stroke care and Comprehensive Stroke Centers
- Community-level investment and structural reforms in underserved urban neighborhoods
For patients and families, these findings also reinforce the importance of recognizing stroke symptoms quickly and calling 911 immediately. Time is brain—yet the system must ensure that “time” and “access” don’t vary based on race, ZIP code, or insurance status.Source: Society of NeuroInterventional Surgery (SNIS), July
Related Links
- Society of NeuroInterventional Surgery (SNIS) — https://www.snisonline.org
- NIH: Stroke (overview, symptoms, treatment) — https://www.ninds.nih.gov/health-information/disorders/stroke
- CDC: Stroke (risk factors, prevention, data) — https://www.cdc.gov/stroke/
- American Stroke Association (ASA): Stroke resources — https://www.stroke.org/
- NIH Stroke Scale (NIHSS) basics (clinical context) — https://www.stroke.nih.gov/resources/scale.htm
- Find a certified stroke center (The Joint Commission) — https://www.qualitycheck.org/
SOURCE Society of NeuroInterventional Surgery
💪 Your health journey starts here! Explore the latest health news, fitness tips, wellness trends, and healthy living advice. Share your thoughts in the comments and subscribe to the STM Daily News newsletter to stay informed and inspired every day.





